


























General - Erythrocytes
Pathological
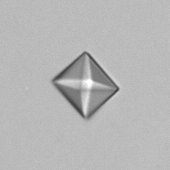
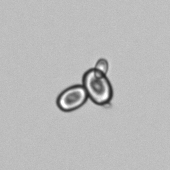
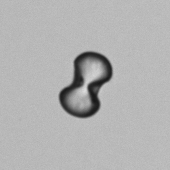
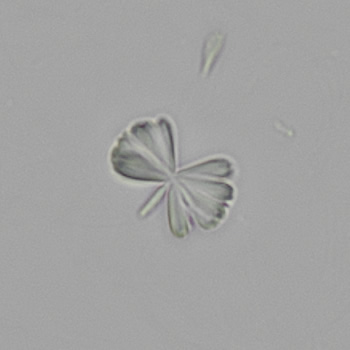
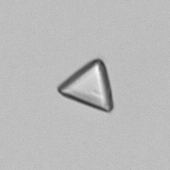
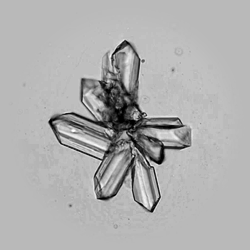
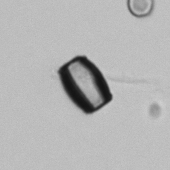
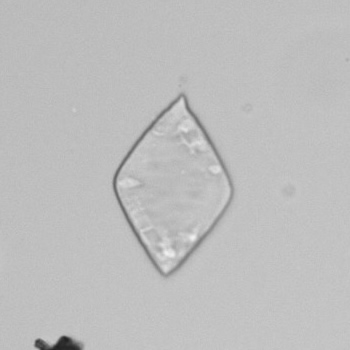
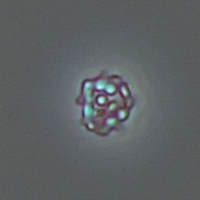
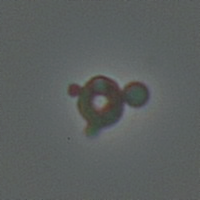
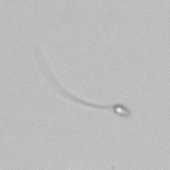
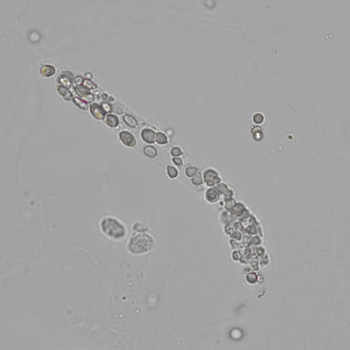
The morphological assessment of erythrocytes in urine plays an important supporting role in determining the cause of hematuria. It distinguishes between nephrogenic (glomerular) and urologic (nonglomerular) causes, based on specific characteristics such as the shape of the erythrocytes (isomorphic versus dysmorphic), the degree of homogeneity (monomorphic versus polymorphic) and the presence of erythrocyte cylinders. In non-glomerular hematuria, the urine sediment is usually monomorphic and the erythrocytes are isomorphic in shape. In contrast, glomerular hematuria is characterized by polymorphism - the occurrence of multiple (more than two) different aberrant erythrocyte forms - combined with dysmorphism and the presence of erythrocyte cylinders.
Indications of a nephrogenic cause of hematuria include a history of renal or systemic disease, a positive family history, relevant clinical complaints and abnormal physical findings. Laboratory tests can further support this suspicion. Important indicators include abnormalities on the urine strip analysis, an abnormal urine sediment with an increased percentage of dysmorphic erythrocytes (>40%), the presence of >5% acanthocytes and/or erythrocyte cylinders, an increased protein/creatinine ratio or albumin/creatinine ratio in the morning urine, and signs of impaired renal function, such as a decreased eGFR or rising serum creatinine.
International guidelines, such as the EFLM European Urinalysis Guideline 2023 (Chapter 6.2.4.4), provide additional information on a systematic approach. These include proper sample collection, rapid processing and standardized reporting, which are essential for reliable interpretation.






